Calprotectin
What this marker measures
Calprotectin is a human protein released primarily by neutrophils during intestinal inflammation and measured in the stool. It helps distinguish inflammatory conditions such as inflammatory bowel diseases (IBD) from non-inflammatory conditions such as irritable bowel syndrome (IBS), and to monitor IBD activity and relapse risk1–3. This assay is issued under the European IVDR framework (the assay is classified IVDR Class C) with ARTG listing for use in Australian markets
Clinical associations*
Consider this marker when your patient presents with:
*In addition to the assay’s intended use, all clinical associations have been reviewed by the Microba science team to ensure clinical validity supported by Microba’s cited literature.
Interpreting the result
All results are compared to Microba's healthy cohort to determine whether they fall within or outside the expected range.
Patient management insights
Investigate the underlying cause of elevated calprotectin. Adjunctive dietary or supplement strategies may be considered only once the clinical context is established.
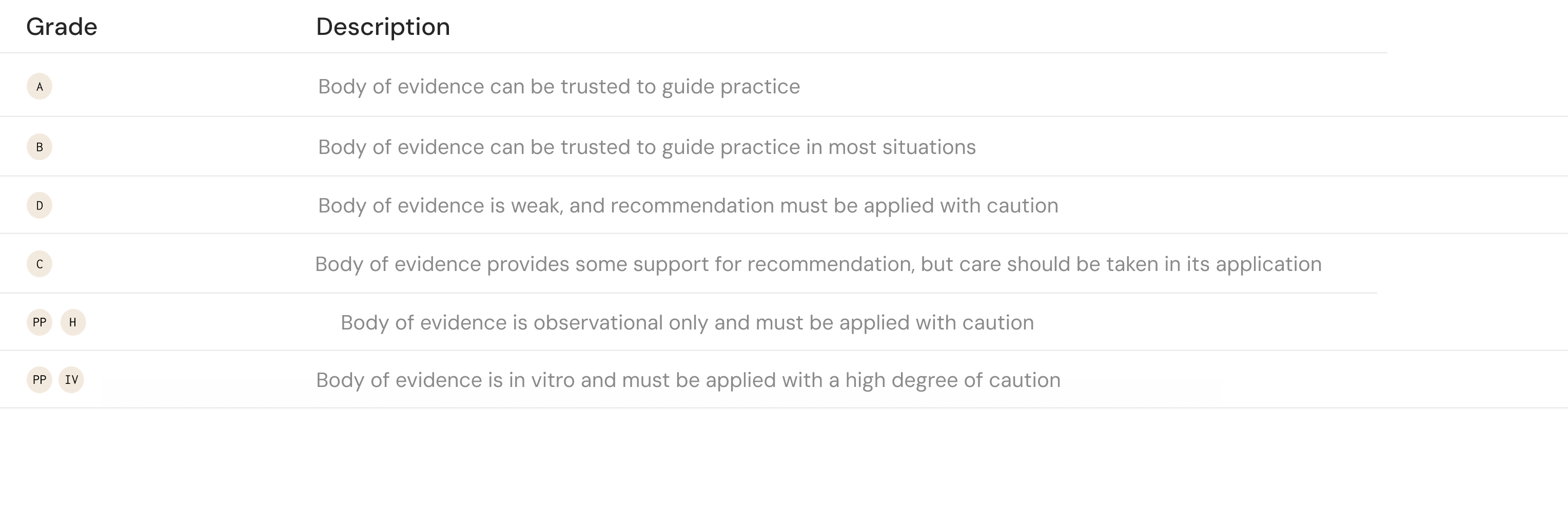
Mediterranean diet as an adjunct to standard therapy, may be associated with lower faecal calprotectin in patients with IBD4–6. GRADE C
Mediterranean diet as an adjunct to standard therapy, may be associated with lower faecal calprotectin in patients with IBD4–6. GRADE C

Tips for discussing out-of-range results
Your result shows elevated calprotectin, which may suggest intestinal inflammation. This does not identify the exact cause, so we’ll review your symptoms, medications, and other test results to decide what next steps are needed.
Calprotectin — Reference sourcesSource references for all clinical associations, interpretation definitions, and patient management insights on this card.
1. Dajti, E. et al. Systematic review with meta-analysis: Diagnostic performance of faecal calprotectin in distinguishing inflammatory bowel disease from irritable bowel syndrome in adults. Alimentary Pharmacology & Therapeutics 58, 1120–1131 (2023).
2. Rokkas, T., Portincasa, P. & Koutroubakis, I. E. Fecal calprotectin in assessing inflammatory bowel disease endoscopic activity: a diagnostic accuracy meta-analysis. J Gastrointestin Liver Dis 27, 299–306 (2018).
3. Mosli, M. H. et al. C-Reactive Protein, Fecal Calprotectin, and Stool Lactoferrin for Detection of Endoscopic Activity in Symptomatic Inflammatory Bowel Disease Patients: A Systematic Review and Meta-Analysis. Am J Gastroenterol 110, 802–819; quiz 820 (2015).
4. Godny, L. et al. Mechanistic Implications of the Mediterranean Diet in Patients With Newly Diagnosed Crohn’s Disease: Multiomic Results From a Prospective Cohort. Gastroenterology 168, 952-964.e2 (2025).
5. Haskey, N. et al. A Mediterranean Diet Pattern Improves Intestinal Inflammation Concomitant with Reshaping of the Bacteriome in Ulcerative Colitis: A Randomised Controlled Trial. J Crohns Colitis 17, 1569–1578 (2023).
6. Chicco, F. et al. Multidimensional Impact of Mediterranean Diet on IBD Patients. Inflamm Bowel Dis 27, 1–9 (2021).
7. Marino, M. et al. A (poly)phenol-rich diet reduces serum and faecal calprotectin in older adults with increased intestinal permeability: the MaPLE randomised controlled trial. BMC Geriatr 24, 707 (2024).
8. Morshedzadeh, N. et al. Effects of flaxseed and flaxseed oil supplement on serum levels of inflammatory markers, metabolic parameters and severity of disease in patients with ulcerative colitis. Complementary Therapies in Medicine 46, 36–43 (2019).
9. Scaioli, E. et al. Eicosapentaenoic Acid Reduces Fecal Levels of Calprotectin and Prevents Relapse in Patients With Ulcerative Colitis. Clinical Gastroenterology and Hepatology 16, 1268-1275.e2 (2018).
10. Prossomariti, A. et al. Short-term treatment with eicosapentaenoic acid improves inflammation and affects colonic differentiation markers and microbiota in patients with ulcerative colitis. Sci Rep 7, 7458 (2017).
11. Banerjee, R. et al. Novel Bioenhanced Curcumin With Mesalamine for Induction of Clinical and Endoscopic Remission in Mild-to-Moderate Ulcerative Colitis: A Randomized Double-Blind Placebo-controlled Pilot Study. J Clin Gastroenterol 55, 702–708 (2021).
12. Lang, A. et al. Curcumin in Combination With Mesalamine Induces Remission in Patients With Mild-to-Moderate Ulcerative Colitis in a Randomized Controlled Trial. Clinical Gastroenterology and Hepatology 13, 1444-1449.e1 (2015).
13. Hanai, H. et al. Curcumin Maintenance Therapy for Ulcerative Colitis: Randomized, Multicenter, Double-Blind, Placebo-Controlled Trial. Clinical Gastroenterology and Hepatology 4, 1502–1506 (2006)
.14. Dryden, G. W., Lam, A., Beatty, K., Qazzaz, H. H. & McClain, C. J. A Pilot Study to Evaluate the Safety and Efficacy of an Oral Dose of (−)-Epigallocatechin-3-Gallate–Rich Polyphenon E in Patients With Mild to Moderate Ulcerative Colitis. Inflammatory Bowel Diseases 19, 1904–1912 (2013).
15. Biedermann, L. et al. Bilberry ingestion improves disease activity in mild to moderate ulcerative colitis — An open pilot study. Journal of Crohn’s and Colitis 7, 271–279 (2013).
16. Zhou, W. Saccharomyces boulardii powder combined with mesalazine for treatment of active ulcerative colitis: Curative effect and impact on fecal calprotectin and serum inflammatory factors. World Chinese Journal of Digestology 25, 2065 (2017).
17. Neyrinck, A. M. et al. Prebiotic dietary fibre intervention improves fecal markers related to inflammation in obese patients: results from the Food4Gut randomized placebo-controlled trial. Eur J Nutr 60, 3159–3170 (2021)
.18. Valcheva, R. et al. Inulin-type fructans improve active ulcerative colitis associated with microbiota changes and increased short-chain fatty acids levels. Gut Microbes 10, 334–357 (2019).
19. Casellas, F. et al. Oral oligofructose-enriched inulin supplementation in acute ulcerative colitis is well tolerated and associated with lowered faecal calprotectin. Alimentary Pharmacology & Therapeutics 25, 1061–1067 (2007).
20. Langmead, L. et al. Randomized, double-blind, placebo-controlled trial of oral aloe vera gel for active ulcerative colitis. Alimentary Pharmacology & Therapeutics 19, 739–747 (2004).