Mucin degrading microbes
What this marker measures
The collective capacity of the microbial community to degrade mucin, the glycoproteins that help form the protective mucus layer lining the gut. Some mucin degradation is normal and may support microbial cross-feeding, but elevated mucin-degrading potential may contribute to mucus layer thinning, reduced gut barrier integrity, and intestinal inflammation, particularly when dietary fibre intake is low1–3.
Clinical associations
Consider this marker when your patient presents with:
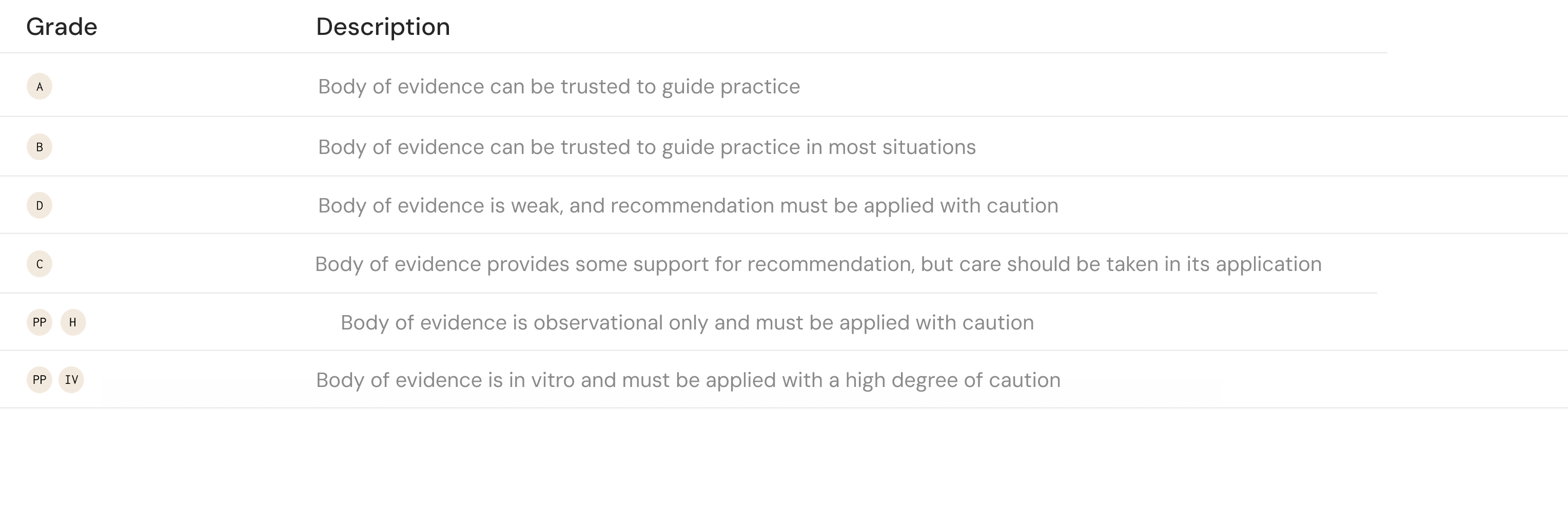
Interpreting the result
All results are compared to Microba's healthy cohort to determine whether they fall within or outside the expected range.
Patient management insights
Reduce excess mucin-degrading potential and support mucus layer and gut barrier integrity.

Tips for patients discussion
Your report shows elevated levels of microbes that can use the gut’s protective mucus layer as a food source. This layer acts as a first line of defence for your intestinal wall. Increasing tolerated dietary fibre can help shift microbial activity toward fibre fermentation and support gut barrier integrity
The community
No single species produces butyrate alone — here are some of the most common, however this list is not exhaustive
- Agathobacter faecis
- Alistipes obesi
- Alistipes onderdonkii
- Alistipes shahii
- Bacteroides caccae
- Bacteroides ovatus
- Bacteroides thetaiotaomicron
- Bacteroides uniformis
- Bacteroides_B vulgatus
- Blautia_A sp900066165
- CAG-41 sp900066215
- Barnesiella intestinihominis
- CAG-56 sp900066615
- Odoribacter splanchnicus
- Roseburia hominis
- Fusicatenibacter saccharivorans
- GCA-900066135 MIC6659
- Roseburia inulinivorans
- Ruminococcus_A sp003011855
- KLE1615 sp900066985
- Parabacteroides distasonis
- Bacteroides_B dorei
- Parabacteroides merdae
- UBA7160 MIC9207
How results are calculated
All microbiome marker results are compared against the Microba Healthy Cohort — a purpose-built reference group of more than 450 healthy individuals, collected and analysed using the same workflow as patient samples.
Each marker is scored by comparing the patient's relative abundance against the cohort average. The distance from this average is expressed as standard deviations, and determines whether a result is classified as Low, Borderline, or High.
Source references for all clinical associations, interpretation definitions, and patient management insights on this card.
1. Blecksmith, S. E., Oliver, A., Alkan, Z. & Lemay, D. G. Gut Microbiome Genes Involved in Plant and Mucin Breakdown Correlate with Diet and Gastrointestinal Inflammation in Healthy United States Adults. The Journal of Nutrition 155, 3757–3768 (2025).
2. Desai, M. S. et al. A Dietary Fiber-Deprived Gut Microbiota Degrades the Colonic Mucus Barrier and Enhances Pathogen Susceptibility. Cell 167, 1339-1353.e21 (2016).
3. Earle, K. A. et al. Quantitative Imaging of Gut Microbiota Spatial Organization. Cell Host & Microbe 18, 478–488 (2015).
4. Pan, S. et al. Gut Microbial Protein Expression in Response to Dietary Patterns in a Controlled Feeding Study: A Metaproteomic Approach. Microorganisms 8, 379 (2020).
5. Dirks, B. et al. Microbial Feast or Famine: dietary carbohydrate composition and gut microbiota metabolic function. bioRxiv 2025.10.27.684932 (2025) doi:10.1101/2025.10.27.684932.